
News | June 29, 2026

The sacroiliac joint is located deep within the pelvis, and when irritated, it often causes pain that patients initially find difficult to identify.
Many people describe the pain as stabbing, pulling, or locking. It’s usually located on one side next to the sacrum and radiates into the buttock, and sometimes into the groin or the back of the thigh. Climbing stairs, sitting for long periods, turning over in bed, or taking that first step after getting out of bed suddenly feel wrong. It’s exactly at this point that people start looking for a solution to relieve the SI joint blockage.
The term sounds mechanical, almost like a jammed hinge. But that’s only partly accurate. While the sacroiliac joint doesn’t move much, it is highly sensitive to tension, improper loading, inflammation, muscular protective responses, and problems in the lumbar spine or hip. Anyone who wants to get their symptoms under control for the long term therefore needs more than just a quick fix.
At ROC Ortho in Aschheim near Munich, we combine orthopedic diagnostics, functional analysis, and regenerative therapy approaches. When it comes to pain in the sacroiliac joint, we believe one question is paramount: Where exactly is your pain coming from?
The sacroiliac joint, or SI joint for short, connects the sacrum to the two iliac bones of the pelvis. It thus forms the bridge between the spine and the legs. Every step, every twist of the torso, and every transfer of weight from the upper body to the hips passes through this region.
The joint has only a small range of motion. This is precisely what protects the pelvic ring, because the sacroiliac joint must provide stability. It glides, tilts, and cushions minimally. These small movements are sufficient to absorb peak loads when walking, bending over, or lifting.
Strong ligaments, deep back muscles, abdominal muscles, the pelvic floor, gluteal muscles, and hip muscles stabilize the joint. If this interplay becomes disrupted, the sacroiliac joint signals pain. Often, there is no significant “displacement.” Rather, a functional disorder develops: muscles tighten, joint surfaces rub against each other, and surrounding nerves become more sensitive.
Lower back pain in the sacroiliac joint resembles symptoms associated with the lumbar spine, the intervertebral discs, the facet joints, the hip, and even irritation of the sciatic nerve. This explains why those affected often alternate between heat therapy, pain relievers, massage, and stretching exercises for a long time without finding a clear solution.
The sacroiliac joint is not easily identified as the source of pain on an X-ray. An MRI can reveal inflammation, stress reactions, signs of osteoarthritis, or other abnormalities, but it does not automatically confirm the source of the pain in everyday life. A physical examination by a doctor therefore remains the first step.
At the ROC, when treating lower back pain, we examine not only the sacroiliac joint but also the lumbar spine, hips, leg alignment, gait, and muscular control. Orthopedic diagnostics at the ROC help clearly distinguish between functional and structural causes.
An ISG block refers to a painful dysfunction in the area of the sacroiliac joint. The joint feels locked, the back compensates by tensing the muscles, and movement triggers pain. The body slows down. Many patients describe this as a blockage in the pelvis.
From a medical perspective, doctors distinguish between functional symptoms, inflammatory causes, degenerative changes, and pain that radiates to the sacroiliac joint from adjacent regions. This classification influences treatment. Resolving acute sacroiliac joint blockage involves a different approach for a functional disorder than for inflammatory sacroiliitis.
A real-life example: A patient spends many hours sitting at work, drives every day, and works out intensely on the weekends. After making a twisting motion while getting out of the car, she feels a sharp pain deep in her back. The sacroiliac joint isn’t solely to blame in this situation. The duration of sitting, hip mobility, core strength, gluteal strength, and daily habits all play a role. The more these factors are reduced, the better the pain can be managed and the function of the thumb maintained in the long term.
Pain in the sacroiliac joint follows a specific pattern that aids in the initial assessment. The pain is often located just next to the sacrum, roughly where many people intuitively press their thumb against the upper buttocks. Doctors refer to this region as the Fortin area.
Symptoms often occur on one side only. They worsen when standing up from a seated position, turning over in bed, doing lunges, climbing stairs, or standing for long periods. Prolonged sitting increases pressure on the sacroiliac joint, especially when slouching slightly.
| Complaint | Characteristic of the sacroiliac joint | Reference to other causes |
|---|---|---|
| Site of pain | deep near the sacrum, often on one side | in the middle of the lumbar spine, severe in the groin, or pronounced in the hip joint |
| Broadcast | Buttocks, groin, back of the thigh | Numbness extending to the foot, loss of strength, electric-shock-like nerve pain |
| Trigger | Standing up, turning, stairs, weight-bearing on one leg | Coughing, sneezing, or straining accompanied by leg pain due to irritation of the intervertebral discs |
| Sense of Movement | Blockage, restriction, feeling of pelvic instability | Hip snapping, groin pain during internal rotation, improper weight-bearing on the knee or foot |
| History | Varies depending on the load and posture | Night pain, fever, weight loss, or signs of inflammation |
This table is not a substitute for an examination. It helps you describe your own symptoms more precisely. It is precisely this description that often provides more clarity during a consultation than a general statement like “lower right back,” which says little about your pain. What matters for treatment is what your hand can do and which symptoms limit you.
Many people search for “how to relieve sciatic nerve blockage” because the pain radiates down their leg. The sacroiliac joint can indeed cause pain that radiates toward the buttocks or thigh. True sciatic pain, on the other hand, is usually caused by irritation of the nerve roots or the sciatic nerve.
The difference matters. Tingling, numbness, loss of strength, or pain that radiates down to the foot or toes requires a medical evaluation of the nerves. If this neurological pattern is absent, the cause is more likely to be local irritation at the sacroiliac joint, the lumbar spine, the piriformis muscle, or the hip.
At ROC, we use electromyography as needed to address neuromuscular issues when symptoms appear to be related to nerve involvement. This helps us avoid prematurely attributing symptoms to the sacroiliac joint when they actually originate from another structure.
Mild discomfort after unusual physical exertion often subsides with movement, warmth, and sensible rest. However, there are situations in which you should not attempt self-treatment.
If you experience these symptoms, you need immediate medical attention. This applies regardless of whether the pain is localized to the sacroiliac joint or radiates to other areas.
Inflammation of the sacroiliac joint—medically known as sacroiliitis—often presents differently than a purely functional disorder. Typical symptoms include deep lower back pain that worsens at rest, wakes the patient at night, and improves with movement. Morning stiffness that persists over a longer period of time is also consistent with an inflammatory pattern.
Such symptoms require a different diagnostic approach. Laboratory test results, MRI scans, and rheumatological evaluation become more important. Simply mobilizing the sacroiliac joint is not enough in such cases. At ROC, we supplement imaging diagnostics with laboratory tests and a structured medical evaluation as needed—for example, through the ROC Laboratory.
When experiencing acute pain in the sacroiliac joint, many people respond by resting. Brief periods of rest help, but lying down for long periods often perpetuates the protective muscle tension. The goal during the first few hours: to alleviate the pain, restore movement, and reduce the alarm response in the nervous system.
Pain relievers should be prescribed by a doctor if you have pre-existing conditions, are taking blood thinners, or have stomach problems, kidney disease, or liver disease. Do not treat medication as a free pass to overexert yourself. Being pain-free while taking pills does not mean that the sacroiliac joint can tolerate a full load.
Lie on your back with your feet hip-width apart. Let your knees sway a few centimeters to the right and left. Keep the movement small. Your pelvis moves slightly along with the motion, and your breathing remains calm. Two minutes is enough to start with.
This exercise is not intended to “pop” the sacroiliac joint back into place. It sends a message to the body that movement is possible. If you experience sharp pain, numbness, or increasing radiating pain, stop the exercise and have a doctor evaluate your symptoms. Diagnosis—and an open discussion about realistic expectations.
Exercises for the sacroiliac joint are most effective when they combine three goals: increasing hip mobility, controlling the core, and activating the gluteal muscles. Individual stretches rarely provide lasting relief if daily life repeatedly subjects the pelvis to the same improper strain.

Get into a half-kneeling position. Place one knee on a soft surface, with the other foot in front. Straighten your upper body and push your pelvis forward slightly until you feel a stretch in the front of your hip. Hold for 30 seconds on each side.
A shortened hip flexor pulls the pelvis forward and alters the load on the sacroiliac joint. Many people with sedentary jobs benefit from this simple correction.
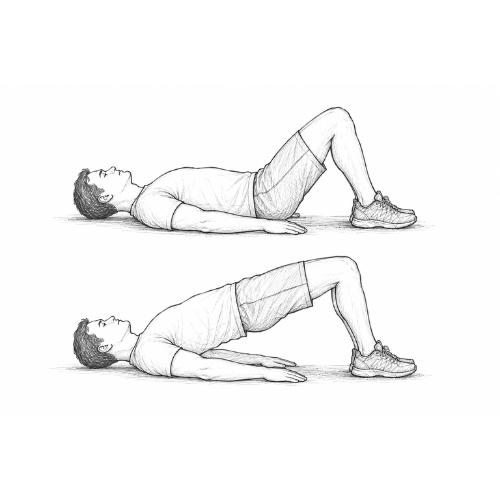
Lie on your back with your feet flat on the floor. Tighten your glutes and slowly lift your pelvis until your thighs and upper body form a straight line. Lower yourself in a controlled manner. Eight to twelve repetitions are sufficient.
The focus is on control. If you feel the movement in your lower back instead of your glutes, lower the height. The sacroiliac joint needs guidance, not a display of strength.
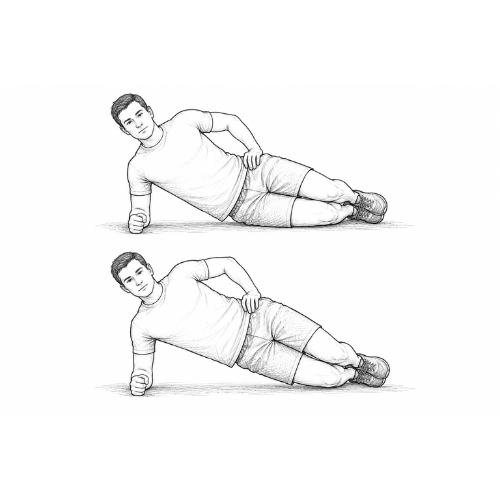
Lie on your side with your knees bent. Support yourself on your forearm and lift your pelvis a few centimeters. Hold for five to ten seconds. Switch sides.
This exercise works the lateral core chain. These muscles stabilize the pelvis and sacroiliac joint when walking, climbing stairs, and standing on one leg.
Stand in front of a mirror. Slowly shift your weight onto one leg without letting your pelvis tilt to the side. Hold this position for three breaths, then switch sides. The mirror will show you if your upper body is leaning to one side.
This exercise may seem unspectacular. However, it provides a lot of information about the sacroiliac joint, since every step consists of short phases on one leg.

If pain returns despite consistent exercise over several weeks, the sacroiliac joint requires a more detailed evaluation. In that case, we assess posture, leg alignment, foot pressure, and spinal movement at the ROC. The 4D spinal analysis in Aschheim shows how the pelvis, spine, and leg alignment work together under load.
Physical therapy is a good option once the acute inflammation subsides. At ROC Physio, medical findings, movement analysis, and exercise are integrated into a comprehensive treatment plan. For patients with recurring pain in the sacroiliac joint, this integrated approach often leads to progress that cannot be achieved through isolated, individual measures.
The sacroiliac joint rarely reveals its role through a single finding. Doctors combine medical history, physical examination, range-of-motion testing, provocation tests, and, if necessary, imaging. The goal is to reproduce the pain, identify patterns, and rule out other causes.
Multiple positive provocation tests increase the likelihood that the sacroiliac joint is involved in the pain. Nevertheless, the finding remains part of the overall picture. A positive test alone does not confirm a diagnosis.
An X-ray shows bone structure, signs of osteoarthritis, or significant misalignments. An MRI detects inflammation, bone marrow reactions, intervertebral disc problems, and many soft tissue abnormalities. An MRI plays an important role in cases of unexplained pain or suspected sacroiliitis.
At the ROC, patients have access to an open MRI scanner in Aschheim. This is particularly helpful for people who want to avoid narrow tubes. Depending on the specific issue, we supplement the evaluation with digital X-rays, ultrasound, or pedobarography and gait analysis.
Hip osteoarthritis, impingement, bursitis, and tendon problems cause symptoms that radiate into the sacroiliac joint. Conversely, a painful sacroiliac joint alters gait and puts strain on the hip. The two conditions influence each other.
A thorough examination therefore assesses hip rotation, groin pain, stride length, and pelvic stability. In cases of advanced osteoarthritis or complex joint problems, we at the ROC incorporate regenerative options and osteoarthritis treatment into the treatment plan, depending on the findings.
Many patients hope for that one adjustment that will relieve the blockage. Manual therapy can alleviate acute functional disorders of the sacroiliac joint, especially when muscle tension, joint instability, and fear of movement are driving the symptoms.
The outcome depends heavily on the diagnosis. In cases of inflammatory sacroiliitis, fracture, infection, cancer, or significant neurological deficits, manipulation of the sacroiliac joint is not indicated. A reputable treatment approach first assesses the risks and causes of pain.
At ROC, we use manual medicine and chiropractic therapy in a targeted manner when the findings and the patient’s condition warrant it. The manual technique is not used in isolation. After mobilization, the sacroiliac joint requires active stabilization; otherwise, the old pattern often returns.
A noticeable cracking sound says little about the success of the treatment. Many joints crack due to gas bubbles in the joint space or tendon movements. What matters most for treatment is the improvement: less pain, better mobility, and a more stable gait.
After manual therapy, we focus on the next step. What kind of movement has been lacking? Which muscles have been compensating? What daily activities are putting strain on the sacroiliac joint again? These questions help prevent patients from having the same blockage treated at every appointment.
Many patients ask for an “sacroiliac joint injection” when pain persists despite exercises, physical therapy, and pain management. An injection delivers medication directly to the affected structures. Depending on the situation, it is used for pain management, to reduce inflammation, or for diagnostic purposes.
During an ISG injection, a precisely targeted injection is administered into the sacroiliac joint or the surrounding area where pain originates. Depending on the procedure, doctors use local anesthetics, anti-inflammatory agents, or other injection techniques. The specific choice depends on the diagnosis, pre-existing conditions, and treatment goals.
At the ROC, we only schedule infiltration therapies after a medical examination. Blind injections without a clear target are not consistent with a high-quality treatment approach. Imaging or ultrasound guidance increase precision when the anatomy and findings warrant it.
If a nerve block at the sacroiliac joint significantly reduces the typical pain, this suggests that this region is involved. If the pain remains unchanged, another cause becomes the primary focus. This diagnostic information is particularly helpful in cases of chronic symptoms.
An injection is no substitute for exercise. It can create a window of opportunity in which exercise, physical therapy, and gradual increase in activity can once again be successful. Without this next step, the benefits often diminish quickly.
Chronic pain in the sacroiliac joint is rarely caused by a single factor. Often, it results from a combination of old injuries, reduced hip mobility, core weakness, stress, lack of sleep, a tendency toward inflammation, and a pain system that has become hypersensitive. While the sacroiliac joint remains the site of the pain, the underlying cause sometimes lies within the entire musculoskeletal and regulatory system.
At this stage, therapy needs structure. Repeated adjustments without analysis often lead to a vicious cycle. Effective treatment asks: Which tissues are sending pain signals? What stress is maintaining the stimulus? What resources does the body lack for healing and adaptation?
| Building block | Goal | When it fits |
|---|---|---|
| Manual medicine | Enable movement, lower the safety voltage | Acute or recurrent functional blockages |
| Physiotherapy | Build stability, coordination, and resilience | after acute pain relief and in the event of relapses |
| 4D Spinal Measurement | Analyze posture, pelvic alignment, leg axes, and gait pattern | Unclear cause of strain, recurring symptoms |
| MRI | Assessing Inflammation, Intervertebral Discs, Bones, and Soft Tissues | Warning signs, chronic course, suspected sacroiliitis |
| Infiltration | Identify the source of pain; soothe the irritation | Persistent localized pain despite conservative treatment |
| Denervation | Targeted Reduction of Pain Transmission | Chronic, clearly localized pain near the joints following testing |
Modern pain medicine does not view the sacroiliac joint in isolation. At the ROC, when treating chronic symptoms, we consider spinal therapy, minimally invasive pain therapy, and regenerative approaches, depending on the findings.
In selected cases of persistent pain originating from structures near the joints, denervation may be considered. In this procedure, doctors treat small pain-conducting nerve branches using radiofrequency technology. The goal is to reduce pain signals from the treated area and restore mobility.
Denervation requires careful assessment of the indications. Before proceeding, physicians identify the source of the pain, often using diagnostic nerve blocks. The procedure is not suitable for every sacroiliac joint, nor for diffuse pain, nor for symptoms whose cause remains unclear.
The ROC offers denervation as part of a broader orthopedic approach to pain management. When indicated, this procedure can help break chronic pain cycles. Afterward, active rehabilitation is essential, as a more stable pain system requires strong muscles and proper movement patterns.
Regenerative medicine draws on the body’s own resources and biological repair processes. When it comes to the sacroiliac joint, it does not offer a blanket promise of a cure. It can be part of an individualized treatment plan for certain degenerative, overuse-related, or joint-related conditions.
At the ROC, what began as an orthopedic practice has evolved into an interdisciplinary center for regenerative medicine. When treating sacroiliac joint disorders, we therefore consider not only joint mechanics but also tissue quality, susceptibility to inflammation, metabolism, load management, and long-term prevention.
Depending on the diagnosis, orthobiological therapies may be used in other joint regions or to address accompanying problems. Examples include autologous blood therapy and PRP in orthobiology, stem cell therapy at the ROC, or combined treatment approaches for osteoarthritis and tendon irritation.
Regeneration begins with the question of which tissue needs support. An irritated sacroiliac joint, inflammatory sacroiliitis, intervertebral disc irritation, and hip osteoarthritis all require different treatment strategies. Anyone who lumps all of these conditions together under the term “sacroiliac joint dysfunction” loses precision.
That is why we first determine whether the sacroiliac joint is the primary cause, a contributing factor, or a secondary issue. Only then do we select a treatment. This approach prevents us from acting hastily and saves valuable time.
The sacroiliac joint responds well to rhythm. Walking, cycling with proper seating posture, moderate strength training, and controlled mobility exercises help many patients. Rapid changes in direction, hard jumps, rotational stress when fatigued, and exercising despite sharp pain can have adverse effects.
When getting back into exercise, it's all about the dose. A pain-free 20-minute walk does more for the sacroiliac joint than an ambitious run that causes stiffness the next day.
Rotational sports place a heavy strain on the sacroiliac joint because the pelvis and trunk work against each other. This isn’t necessarily a bad thing. It becomes problematic, however, in cases of limited hip mobility, a weak lateral core, or a lack of recovery.
For patients who are physically active, we assess their gait, foot pressure, and pelvic movement at the ROC as needed. The golf medicine clinic is a good fit if you experience sacroiliac joint pain during your swing, rotation, or longer rounds.
Pain originates in the tissues and the nervous system. Lack of sleep, high work-related stress, insufficient rest, and constant tension increase baseline sensitivity. The sacroiliac joint then reacts more quickly to stresses that were previously tolerable without any problems.
That doesn’t mean the pain is “psychological.” It means that your body interprets stimuli more intensely when your energy reserves are depleted. In treating chronic SI joint symptoms, we therefore take into account physical stress, exercise, nutrition, sleep, and autonomic nervous system regulation.
The ROC offers additional tools, such as VNS analysis, when recovery, stress regulation, and performance are factors in the course of therapy. For appropriate cases, IHHT altitude training complements medical care.
Patients often come in with a clear expectation: they want their sacroiliac joint to start functioning properly again as soon as possible. We understand that. At the same time, an accurate diagnosis helps prevent unnecessary treatments and recurring flare-ups.
We ask about the location of the pain, whether it radiates, when it started, physical activity, sports, occupation, previous injuries, surgeries, medications, and warning signs. Your description often points us in the right direction. Where exactly is the pain located? What triggers it? What relieves it?
The sacroiliac joint is the focus of our attention, but it is not the only area we examine. We assess the lumbar spine, hip joints, muscle chains, leg alignment, reflexes, and sensitivity. This allows us to determine whether a sacroiliac joint blockage is a plausible cause or whether the intervertebral disc, hip, facet joints, or nerves are the primary areas of concern.
Depending on the findings, we use open MRI, digital X-rays, ultrasound, 4D spinal measurement, or gait analysis. If inflammation is suspected, laboratory tests are used to supplement the evaluation. Bone density testing is important when osteoporosis, fracture risk, or weight-bearing bone pain are a concern.
Acute symptoms require relief. Recurring symptoms require addressing the underlying causes. Chronic pain requires a step-by-step approach. That is why, depending on the situation, we combine manual medicine, physical therapy, injections, regenerative therapy, pain management, exercise, and prevention.
If you would like to have your sacroiliac joint symptoms evaluated in detail, please plan your visit by checking the directions to the ROC in Aschheim or learn more about the services and organizational procedures at ROC Ortho.
Rest provides short-term relief. After a few days, however, the body loses its resilience, muscles tense up more, and movements feel more threatening. The sacroiliac joint needs gradual movement as soon as warning signs have been ruled out.
Many people pull aggressively on their buttocks or the back of their thighs. This can further aggravate an already irritated area. Stretching the sacroiliac joint should be done gently, slowly, and with minimal pain.
The sacroiliac joint is at the center of a chain. The feet, knees, hips, trunk, and thoracic spine all influence the load placed on it. Local treatment often provides acute relief but is rarely sufficient in cases of recurrence.
Radiation does not automatically mean nerve damage. Nevertheless, numbness, loss of strength, and widespread sensory disturbances require a neurological examination. Accuracy prevents incorrect treatment.